You are asked to examine a previously healthy 5-year-old boy who was just admitted
because of the sudden onset of arm and leg weakness.
His illness began 5-days before admission when he developed a low-grade fever, rhinorrhea,
a sore throat and an intermittent dry cough. On the day of admission, while his respiratory
illness appeared to be resolving, he developed a headache and an abrupt onset weakness
in his right arm and left leg. He also said he had "trouble" seeing.
His epidemiological history is pertinent in that several of his family members had
experienced a similar respiratory illness prior to his becoming ill. The child is
fully immunized to whooping cough, chicken pox, measels, mumps and polio. The family
owns one dog, two cats, and a domesticated weasel. There has been no recent travel.
His general examination, including his vital signs, is normal except for mild injection
of his oropharynx. Neurological examination reveals slight meningismus, weakness of
cranial nerve 6 bilaterally, and grade 4 (no movement) weakness of his right arm and
grade 3 (movement but not against gravity) in his left leg. Deep tendon reflexes are
absent in the affected extremities. There is no sensory loss.
His complete blood count is normal except for a slight neutrophilia. His metabolic
panel is normal. A lumbar puncture reveals a normal opening pressure, clear CSF, a
protein of 85 mg/dL, a pleocytosis of 100 cells 95% of which are mononuclear, a normal
glucose, and negative stains (Grams, acid fast and silver methenamine). CSF serology
is pending.
What is your diagnosis, what test(s) would you order to confirm your diagnosis, and
what treatment, if any, do you recommend?
DIAGNOSIS: Acute flaccid myelitis (AFM). AFM is a disabling polio-like illness primarily
affecting children. Outbreaks of the disease, which is caused by non-polio enteroviruses
(primarily EV-D68) have been documented globally since 2012. The disease is characterized
by the sudden onset of flaccid weakness in one or more limbs. Trunk, neck, respiratory,
bulbar, facial and extraocular muscles can also be affected. Eighty-five to 95% of
AFM patients will have experienced a prodromal fever and/or a cold-like illness.
The cerebrospinal fluid in AFM is typical of an "aseptic meningitis" with negative
bacterial and fungal cultures and stains, a predominantly lymphocytic pleocytosis,
a moderately elevated protein, and a normal glucose level. MRIs show grey-matter abnormalities
in the motor regions of the spinal cord in keeping with the physical examination findings
of lower motor neuron disease (flaccid weakness, hyporeflexia or arreflexia). Stool
cultures should be done to isolate the enterovirus and to rule out poliomyelitis.
Following recovery of the acute illness, patients with AFM typically have substantial
residual disability and long-term rehabilitation needs.
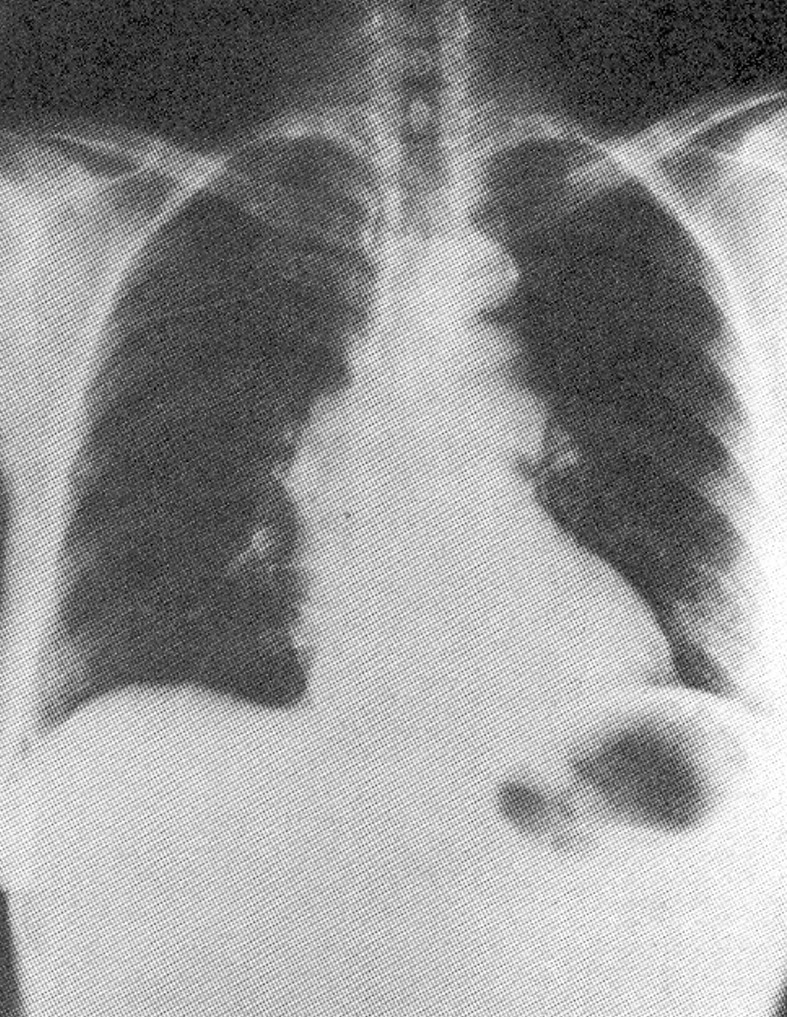
BONUS QUESTION ANSWER: Coarctation of the aorta. The chest x-ray shows a classic "3" sign in the aorta
(the aortic arch, the constriction, and the post-stenotic dilation).
To receive credit please email your answers to smithj@etsu.edu