You are on your emergency room rotation and are asked to make a diagnosis in a 32-year-old
woman who presents with a skin rash and a persistent generalized headache of two days
duration. She has been running a fever associated with true rigors. She lives in a
wooded area of a rural community. On physical examination, she is acutely ill with
a temperature of 38.5 degrees centigrade, respirations of 14/minute, and a pulse rate
of 98 beats per minute. Her blood pressure is normal. Her physical examination is
notable for the rash (see below) and mild nuchal rigidity.
DIAGNOSIS: Lyme borreliosis manifested in the presented case by a characteristic skin rash
(a "target" lesion) and by neuroborreliosis (i.e., aseptic meningitis).
Lyme borreliosis is the most common tick-borne disease in North America. It is caused
by the spirochaete Borellia burgdorferi and is most commonly transmitted by deer ticks that have remained attached to the
skin for at least 36 hours. Small mammals such as mice and voles and rarely, birds
serve as the main reservoir of the organism.
Acutely ill patients may present with neuroborelliosis (aseptic meningitis, encephalitis,
myelitis, Bell's palsy, and/or radiculitis), myocarditis (typically manifested by
varying degrees of heart block), and/or pericarditis. Late manifestations include
arthritis and skin manifestations (acrodermatitis chronica atrophicans). The diagnosis
can be confirmed by measuring acute and convalescent antibody levels. The organism
is sensitive to a variety of antibiotics including tetracyclines, amoxacillin, and
second and third generation cephalosporins. The preferred treatment of uncomplicated
cases is doxycycline 500 mg a day for 10 days.

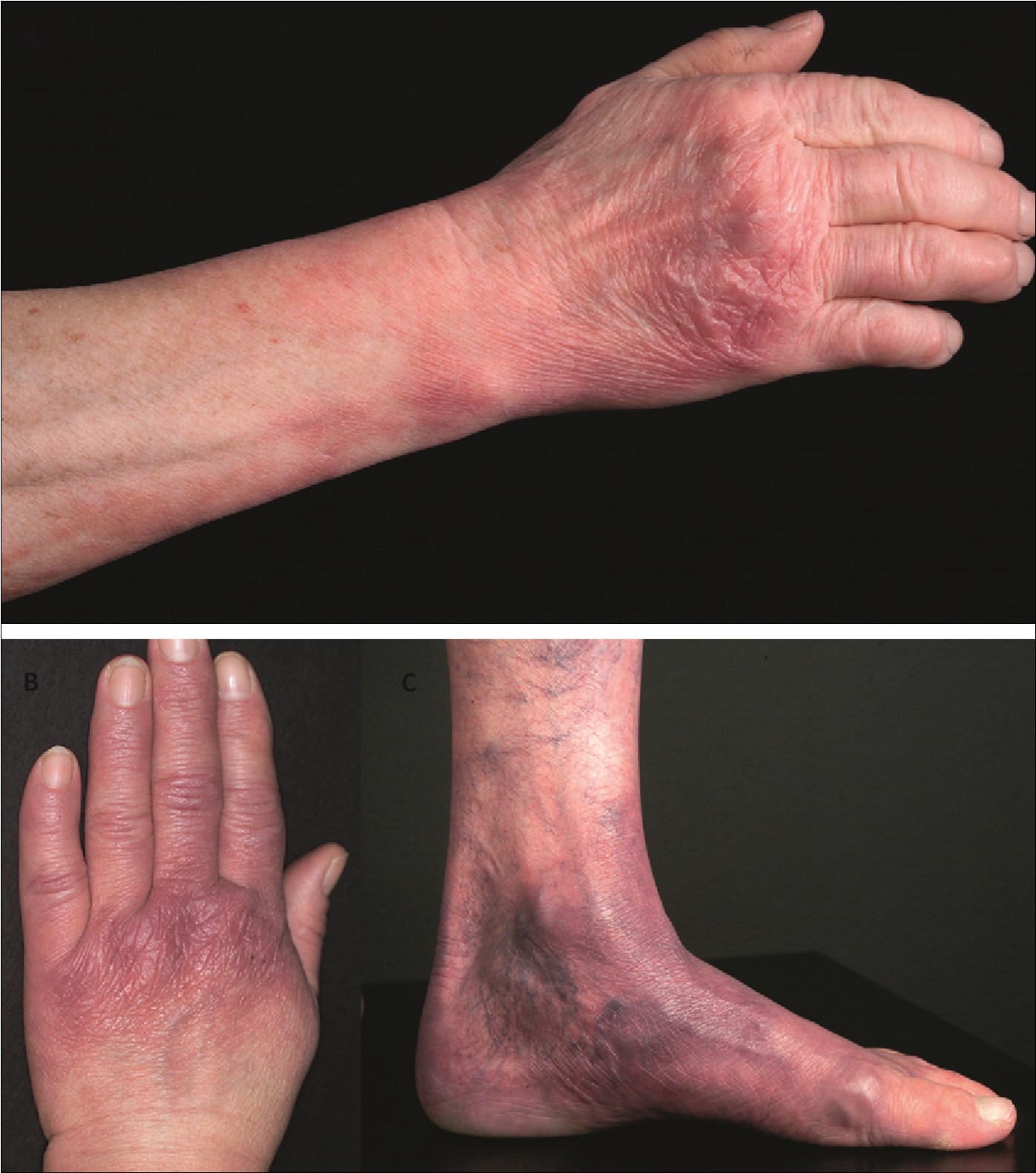
A typical "target" lesion of acute Lyme disease Acrodermatitis chronica atrophicans
.