Last Week's Medical Mystery
You are rotating on the medical service and are asked to evaluate a 65-year-old
man who presents with a chief complaint of "I have lost some vision in my right eye".
His past medical history is positive for Type II diabetes, hypertension, hyperlipidemia,
and for smoking 1-2 packs of cigarettes a day for 40 years.
On physical examination he is tachypneic and hyperpneic. He has fine inspiratory
crackles at both bases posteriorly. You note a positive Kussmaul sign and a left border
of cardiac dullness that is 11-12 cm from the midsternal line in the 5th intercosal
space. A summation gallop is present. He has diminished sensation in his fingers and
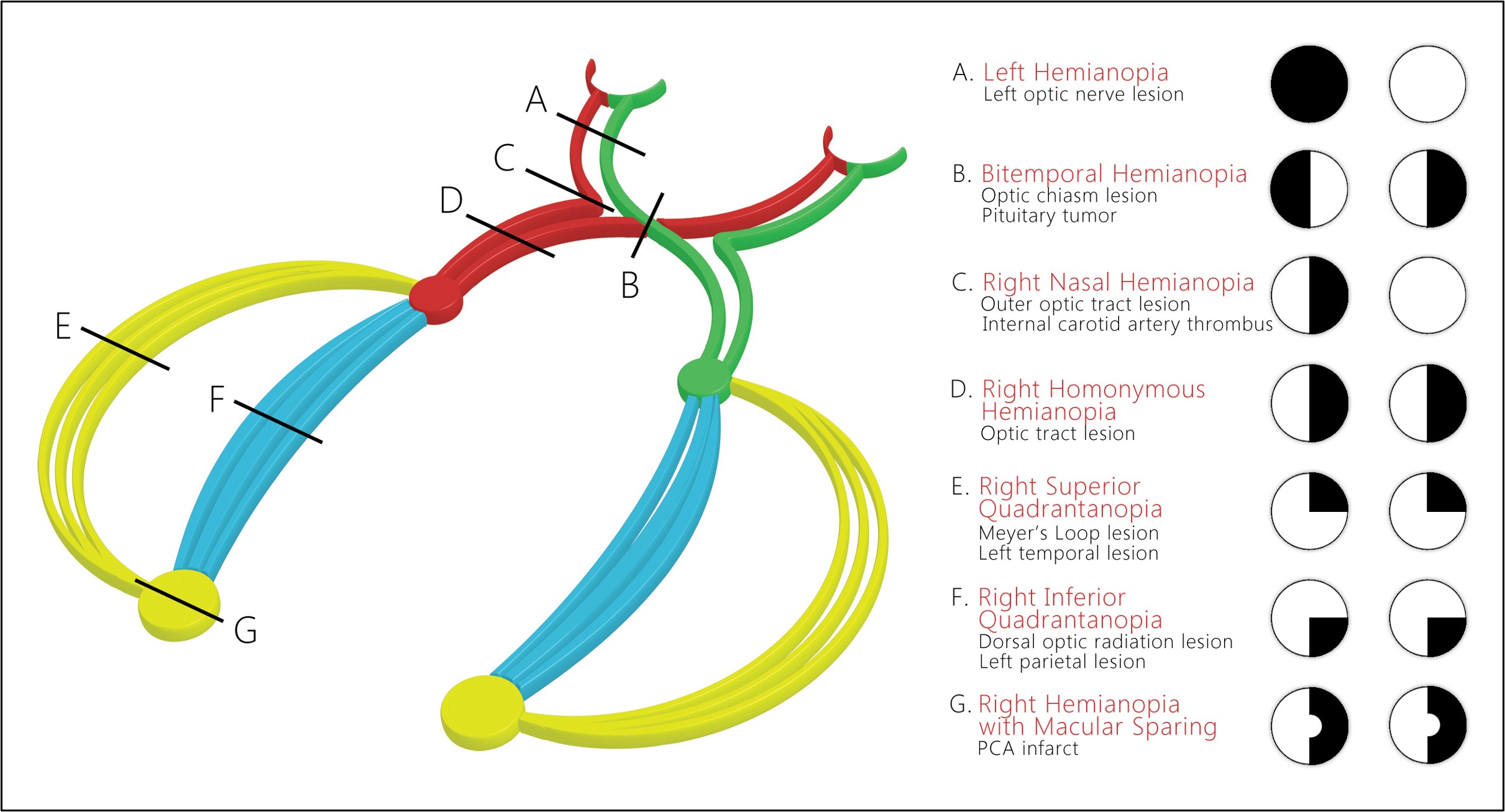
toes. On ophthalmalogical examination, you note a right superior quadranopia. His
chest x-ray and EKG are shown below. Your attending physician asks you the following
questions:
1. Using the American Heart Association's classification of heart disease, what are
his cardiac diagnoses?
2. What part of the brain has been damaged to account for his visual defect?
DIAGNOSES:
AHA Classification of Heart Disease: I. Etiology: coronary heart disease; 2. Anatomy:
anterioseptal myocardial infarction; 3. Physiology: congestive heart failure; left
bundle branch block, RV pacing; Class: IVD.
His right superior quandrantanopia is due to a CVA involving the left temporal region
of his optic radiation (Myers Loop) (see below), probably secondary to poorly controlled
hypertension.
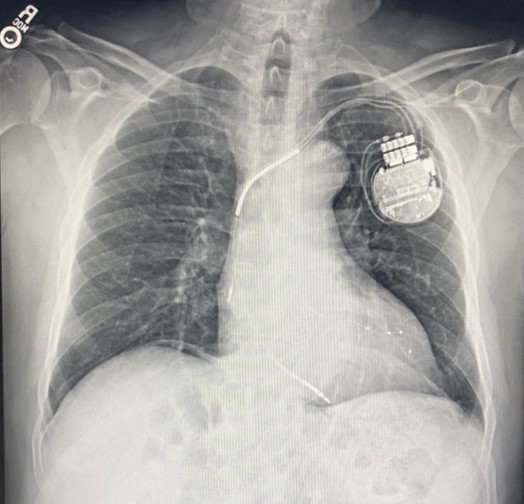
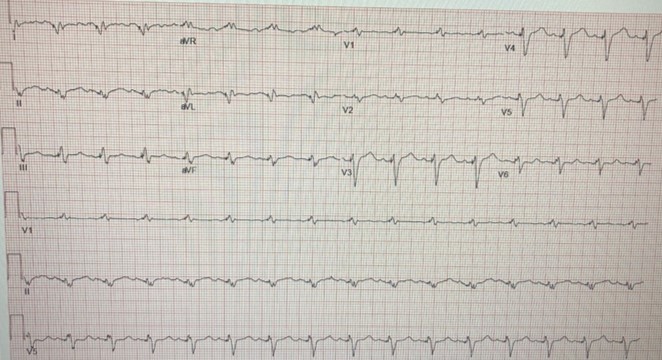
The chest x-ray shows the pacemaker with leads in the right ventricle, borderline cardiomegaly, a prominent aortic knob, and an increase in interstitial markings. The EKG shows a paced rate of 100 beats/minute, Q waves in leads I and II and poor R wave progression in leads V1 and V2 indicating a past anteriorseptal myocardial infarction; also present is evidence of a left bundle branch block.
.